Tendon transfers can be a great option for many patients who have significant injury to the rotator cuff but may want to avoid reverse shoulder replacement. Tendon transfers may be less invasive than replacement surgery and are a permanent repair with fewer restrictions on future activity. There is also less risk of additional surgeries in the future, such as with patients who undergo joint replacement at a young age.
Tendon transfers can help restore motion to the shoulder, but they don’t resolve any pain associated with arthritis. Thus, tendon transfers are typically done for patients with minimal or no arthritis. For patients with arthritis and an irreparable rotator cuff tear, reverse shoulder replacement surgery is usually the better option.
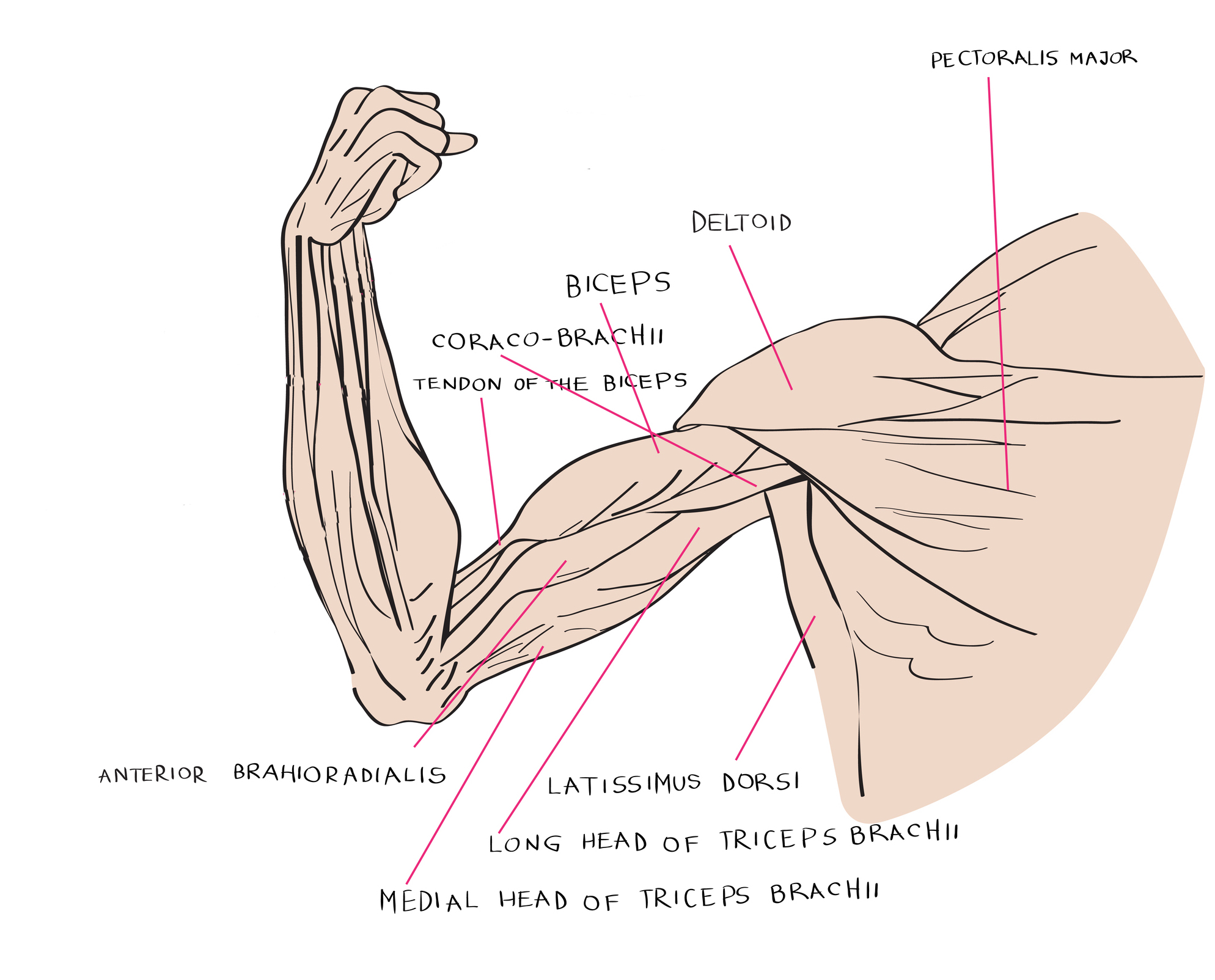
Here we review three major tendon transfers for the shoulder: latissimus dorsi, pectoralis major, and lower trapezius. In these procedures, the tendon is detached from its regular location and moved to a new location, which changes the force vector to allow it to move the shoulder in a different way. Tendon transfers can be particularly useful for patients who are younger or have a job that requires heavy labor and hope to avoid reverse shoulder replacement.
In some cases, a tendon transfer is done along with a shoulder replacement surgery. For example, a latissimus dorsi tendon transfer can be done alongside or in combination with teres major transfer (called a modified L’Episcopo procedure) while doing a reverse shoulder replacement in a patient with profound weakness that limits external rotation.
A latissimus dorsi transfer is used in patients whose rotator cuff tear is irreparable and located in the posterosuperior position of the rotator cuff, which results in pain and weakness in external rotation. One quick test for this type of injury is the hornblower sign, during which the arm is lifted with the elbow at 90 degrees and the hand pointed up. If the hand falls in the fashion of a hornblower, that can signal that the part of the rotator cuff responsible for external rotation is too weak and the patient might be a candidate for tendon transfer.
The latissimus dorsi transfer was first developed by Dr. Christian Gerber in Switzerland, whom Dr. Betsy Nolan studied under during her first shoulder and elbow fellowship. The procedure requires incisions in the front and back of the shoulder and generally requires three to six months of specialized physical therapy afterward to train the muscles to work in a new way.
A lower trapezius tendon transfer can be done arthroscopically but works similarly to a latissiumus dorsi transfer. Both eliminate the restrictions required with joint replacement.
The pectoralis major transfer treats a different type of rotator cuff tear, a tear of the subscapularis tendon in the front. The procedure helps restore internal rotation to the shoulder, which impacts daily activities like tucking in a shirt or getting a wallet out of a back pocket. If the tendon can be repaired, then a primary repair is done. In patients whose subscapularis tendon is not repairable, a pectoralis major tendon transfer may be an option.
It is common that a surgeon may offer some, but not all, of these treatment options, depending on their skill set. If you have an irreparable rotator cuff tear and want to be able to consider all of your treatment options, contact us today at the Oklahoma Shoulder Center to schedule a consultation.
By Oklahoma Shoulder Center PLLC
August 30, 2017
Blog Posts